-
Categories
-
Pharmaceutical Intermediates
-
Active Pharmaceutical Ingredients
-
Food Additives
- Industrial Coatings
- Agrochemicals
- Dyes and Pigments
- Surfactant
- Flavors and Fragrances
- Chemical Reagents
- Catalyst and Auxiliary
- Natural Products
- Inorganic Chemistry
-
Organic Chemistry
-
Biochemical Engineering
- Analytical Chemistry
- Cosmetic Ingredient
-
Pharmaceutical Intermediates
Promotion
ECHEMI Mall
Wholesale
Weekly Price
Exhibition
News
-
Trade Service
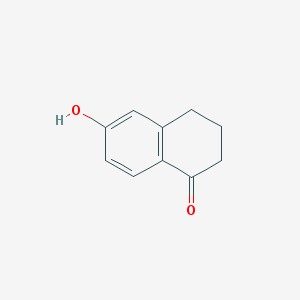
On July 25,, the FoodDrugAdministration (FDA) approved safety label corrections that showed 0.06 percent estroGel; Ascend Therapeutics, Incto increase the risk of stroke, deep vein thrombosis, endometrial cancer and breast cancerEstrogen therapy should be limited to the lowest effective dose and the shortest treatment time corresponding to the treatment targetAccording to the study of 10,739 menopausal women aged 50 to 79 in the Women'sHealthCare Initiative (WHI), the trial group that administered 0.625 mg of compound estrogen per day increased the risk of stroke by 6.8 years compared to placebos(Relative risk (RR), 1.39; 95% confidence interval (CI), 1.10 - 1.77; absolute risk per 10,000 women- year, 44 to 32)This increased risk is observed in the first year and beyondThe combination estrogen monotherapy increased the risk of deep vein thrombosis by 7.1 years (RR, 1.47; 95% CI, 1.04 - 2.08; absolute risk per 10,000 women, 23 vs15); and no statistically significant difference in risk of pulmonary embolism compared to the placebo groupIn contrast, the combined use of progesterone significantly increased the risk of deep vein thrombosis (26 to 13 per 10,000 women) and pulmonary embolism (18 to 8 per 10,000 womenThese increased risks were observed in both the previous two years of treatmentArterial vasculardiseasesrisk factors (e.ghigh blood pressure
, diabetes, smoking, high cholesterol, obesity, etc.), risk factors for venous vascular embolism (e.gpersonal or family history of venous vascular embolism, obesity and systemic lupus, etc.) or both should be properly consideredIf possible, estrogen therapy should be discontinued for 4 to 6 weeks before performing surgery that may increase the risk of vascular embolism or cause long-term inactivityThe use of non-aggressive estrogen in women with a complete uterus also increased the risk of endometrial cancer by 2 to 12 times compared to non-drug groupsThe greatest risk observed in patients after they are on medication and medication is 5 to 10 years or more of treatment (15 to 24 times)The risk will last at least 8 to 15 years after treatment is discontinuedWomen receiving estrogen monotherapy recommend clinical monitoring to use appropriate diagnostic methods (including endometrial sample indicators) to eliminate malignanttumorsin the event of undiagnosable persistent or recurrent abnormal vaginal bleedingThe Food
DrugAdministration says extra use of progesterone in menopausal women who undergo estrogen therapy reduces the risk of endometrial hyperplasia, which can lead to endometrial cancer" The findings and observations of the Women'sHealth Care Initiative (WHI) study show that patients who receive the compound estrogen plus progesterone increase the risk of breast cancer, but those who receive estrogen monotherapy have a lower risk In both cases, the risk increases when continued treatment increases and the baseline value returns to the baseline value after 5 years of discontinuation However, the risk of using only estrogen is smaller and occurs later The Food and Drug Administration recommends that all women have a monthly breast self-examination and that clinical health care a breast test every year Chest tumor X-ray screening based on the patient's age, risk factors, and previous mammograms Estradiol gels are used for the treatment of moderate severe vascular constriction and moderate severe menopausal vaginal and vulvaa atrophy