-
Categories
-
Pharmaceutical Intermediates
-
Active Pharmaceutical Ingredients
-
Food Additives
- Industrial Coatings
- Agrochemicals
- Dyes and Pigments
- Surfactant
- Flavors and Fragrances
- Chemical Reagents
- Catalyst and Auxiliary
- Natural Products
- Inorganic Chemistry
-
Organic Chemistry
-
Biochemical Engineering
- Analytical Chemistry
- Cosmetic Ingredient
-
Pharmaceutical Intermediates
Promotion
ECHEMI Mall
Wholesale
Weekly Price
Exhibition
News
-
Trade Service
As we all know, endocrine therapy is one of the effective treatment methods for hormone receptor-positive (HR+) breast cancer, but drug resistance, patient intolerance and poor compliance after long-term endocrine therapy are the main challenges facing clinical practice, so more efficient and better tolerated endocrine therapy drugs
are urgently needed.
It is exciting to note that in recent years, oral estrogen receptor downregulation (SERD) represented by Giredestrant has made many breakthroughs, which is expected to change the treatment landscape
of HR+ breast cancer.
In this regard, Yimaitong specially invited Professor Wang Xiaojia from the Cancer Hospital of the University of Chinese Academy of Sciences to share with us the current status of HR+ breast cancer treatment, the research progress of new oral SERD and the breakthrough road
of HR+ breast cancer treatment.
Professor Wang Xiaojia
Ph.
D.
, Postdoctoral Supervisor, Chief Physician (Level II)Assistant to the President and Director of the Department of Breast Medicine of the Affiliated Cancer Hospital of the University of Chinese Academy of Sciences/Zhejiang Provincial Cancer Hospital
Deputy Director of Zhejiang Cancer Intelligent Diagnosis and Molecular Technology Research Center
Vice Chairman of the Breast Cancer Expert Committee of the Chinese Society of Clinical Oncology (CSCO).
Member of the Standing Committee of the Breast Cancer Professional Committee and the Standing Committee of the Medical Ethics Committee of the Chinese Anti-Cancer Association
Member of the Oncology Cardiology Group of the Cardiovascular Disease Branch of the Chinese Medical Association
Vice President of Yangtze River Delta Cancer Specialist Alliance
Chairman of Zhejiang Breast Cancer Quality Control Expert Committee
Chairman of the Medical Oncology Branch of Zhejiang Medical Association and Vice Chairman of the Pain Branch
Chairman of the Breast Cancer Professional Committee of Zhejiang Anti-Cancer Association and former chairman of the Medical Oncology Committee
Vice President of Zhejiang Society of Immunology (Former Chairman of the Professional Committee of Tumor Immunology and Biotherapy)
Vice President of Zhejiang Translational Medicine Association and President of Precision Medicine Branch
Yimaitong: As an authoritative expert in the field of breast cancer, how do you view the current treatment status of HR+ breast cancer in China? What do you think are the unmet clinical needs today?
Professor Wang Xiaojia
HR+ breast cancer is the highest subtype of all breast cancers, accounting for about
60% of breast cancer patients in China.
Overall, HR+ breast cancer grows slowly, has a relatively good prognosis, can survive with tumors for a long time compared with other subtypes, and has a good effect on endocrine therapy, so HR+ breast cancer patients account for the vast majority of patients in clinical practice, and it is also a patient population
that clinicians focus on.
However, relatively few endocrine therapy drugs are currently available in clinical practice, mainly including selective estrogen receptor modulators (SERMs, such as tamoxifen), aromatase inhibitors (AI), and SERDs (such as fulvestrant).
In the treatment of HR+ breast cancer, it is necessary to combine an endocrine therapy drug
related to the estrogen signaling pathway.
This also results in relatively few drugs available for the post-line treatment of HR+ breast cancer, and it may be necessary to choose a previously used endocrine therapy drug
.
In addition, many patients with HR+ breast cancer may have mutations in genes such as ESR1 after the failure of AI or fulvestrant therapy, and even more pathway mutations after the failure of CDK4/6 inhibitor treatment, and the abundance of gene mutations is often higher, which makes it difficult
to choose subsequent endocrine treatment options.
As shown in the MAINTAIN study¹, the effectiveness of switching to CDK4/6 inhibitors decreased significantly, only 6~8 months
.
Through genetic testing tools such as next-generation sequencing, the information of mutation pathways and abundances can be obtained, targeted drugs can be selected, and endocrine therapy can be combined to make these patients have better survival benefits
.
However, only changing one drug, the actual clinical treatment of HR+ advanced breast cancer can not be better satisfied, if you can, it is best to change a new endocrine therapy drug at the same time as changing the targeted drug
.
This year, ESMO announced the results of two studies of a new and highly effective oral SERD Giredestrant, namely the early CoopERA study and the late acelERA study.
Professor Wang Xiaojia
At present, new oral SERD drugs such as Giredestrant have become a hot spot
in clinical research.
Because after AI, fulvestrant is a very important choice in single-agent endocrine therapy, but intramuscular injection has certain limitations: first, injections on both buttocks will bring anxiety to patients and lead to poor compliance; Secondly, the real effective dose was not reached, the dosage was increased from 250 mg to 500 mg, and the patient's blood concentration was still relatively low, and the steady-state blood concentration could not be reached after 1 month of administration²
.
Therefore, new oral SERD drugs are expected to meet current clinical needs
.
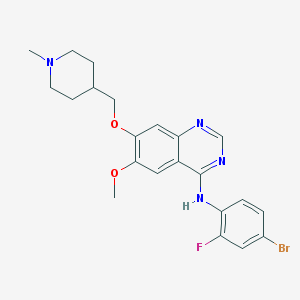
Giredestrant (GDC-9545) is a highly potent non-steroidal oral SERD that, by binding strongly to ER, causes ER to be unable to activate transcription of targeted genes and promotes ER protein degradation, thereby more thoroughly blocking ER signaling and inhibiting tumor cell proliferation³
.
Preclinical studies have shown that Giredestrant has been exposed to 6 times as much as fulvestrant, and 30 mg can achieve near-complete ER binding (>90%), which fully demonstrates its complete antagonistic character and can act on ER mutations associated with drug resistance²⁻⁶
.
Giredestrant supports once-daily oral administration and, at a dose of 30 mg, is well tolerated by patients and has shown good clinical benefit
.
The CoopERA study⁷⁻⁹ and the acelERA study¹⁰ are two key studies
from Giredestrant.
coopERA is a randomized phase II study
using Giredestrant plus pibocicilil versus anastrozole plus perbociclib in the neoadjuvant treatment of ER+/HER2-untreated postmenopausal early stage breast cancer.
A total of 221 patients with ER+/HER2-untreated postmenopausal breast cancer with baseline ki67≥5%
were included in the study.
Patients 1:1 were randomized to the Giredestrant group versus the anastrozole group
.
The Giredestrant group received 2 weeks of Giredestrant monotherapy followed by 16 weeks of Giredestrant plus pibociclib neoadjuvant therapy; The anastrozole group received 2 weeks of neoadjuvant treatment with anastrozole followed by 16 weeks of neoadjuvant therapy
with prastrozole plus pipercillide.
The primary endpoint was change
from baseline in week 2 of the center's assessment.
This year, ASCO updated the final analysis data of coopERA BC⁸, showing that the inhibitory effect of Giredestrant on Ki67 observed at week 2 was greater than that of anastrozole (75% vs 67% of the geometric mean of Ki67 decline from baseline, respectively), with a P value of 0.
0433, which was statistically significant, and the study met the primary endpoint
.
The geometric mean of the decrease in Ki67 from baseline was maintained with surgery with the addition of pipebociclib (81 versus 74 percent).
The safety data were consistent with the known safety profile of Giredestrant, with similar
rates of adverse events (AEs) in both groups.
This is the first randomized controlled study to confirm that Giredestrant is superior to anastrozole
.
Results of the coopERA biomarker subgroup analysis were published at ESMO⁹ In multiple clinical subgroups, Giredestrant treatment significantly reduced Ki67 for 2 weeks compared with the anastrozole group, especially in clinically high-risk groups such as higher stages of AJCC (geometric mean of Ki67 percent decrease from baseline 74.
3 versus 61.
7 percent), clinical lymph node positive (79 versus 59.
3 percent), and PgR negative (60.
1 versus 39 percent) ) and other high-risk features in the tumor subgroup
.
Fig.
1 Results of Ki67 changes in week 2 of coopERA biomarker subgroup analysis
As expected, Giredestrant significantly reduced ER protein levels compared with anastrozole (-42 versus 32 percent), and PgR levels in the Giredestrant group showed a greater downward trend than in the anastrozole group (-48 versus -42 percent).
。 In addition, a stronger tendency was observed in tumors with high-risk features (G3, cN1+) to reduce ER pathway activity in Giredestrant compared with anastrozole (G3 subgroup: ER activity score change -0.
88 vs -0.
64; cN1+ subgroup: -0.
77 vs -0.
63), respectively).
These data provide a basis
for further evaluation of Giredestrant in the adjuvant phase of ER+ breast cancer.
Fig.
2 Changes in ER/PgR protein levels in week 2 of coopERA biomarker subgroup analysis
Fig.
3 Results of ER activity score changes in coopERA biomarker subgroup analysis
The acelERA study is a phase II study
comparing Giredestrant with physician-selected endocrine monotherapy in patients with previously treated ER+/HER2– locally advanced or metastatic breast cancer (LA/mBC).
A total of 303 patients with LA/mBC who had previously received first- or second-line systemic therapy were enrolled with investigator-assessed progression-free survival (PFS)
as the primary endpoint.
This year ESMO published the preliminary analysis results of the acelERA BC study¹⁰
.
Approximately 39% of patients had an ESR1 mutation at baseline; 71% of patients had previously received first-line therapy
.
Seventy-five percent of the patients in the control group received physician-selected endocrine monotherapy fulvestrant at a median follow-up of 7.
89 months, and the median PFS assessed by investigators in the Giredestrant group versus physician-selected endocrine monotherapy group was 5.
6 months and 5.
4 months, respectively, with an HR of 0.
81, although PFS did not reach statistical significance, but the value was slightly higher than that of the physician-selected endocrine monotherapy group
。 Moreover, the Giredestrant group had better benefits
in patients treated with CDK4/6 inhibitors (HR 0.
8), fulvestrant (HR 0.
65), and visceral disease (HR 0.
77).
Fig.
4 PFS results evaluated by investigators in the acelERA BC study
It is worth noting that in the ESR1 mutated population (AI-resistant population), the median PFS of the two groups was 5.
3 months and 3.
5 months, respectively, and the HR was 0.
60, which showed a significant numerical improvement
.
Furthermore, the secondary efficacy endpoints clinical benefit rate (CBR, 31.
8 versus 21.
1 percent) and objective response rate (ORR, 12.
6 versus 7.
2 percent) in the Giredestrant group were numerically superior to the physician-selected endocrine monotherapy group
.
In addition, in terms of safety, Giredestrant is well tolerated, with a safety profile comparable to that of the control group and consistent
with known endocrine therapy risks.
The incidence of grade 3/4 treatment-related adverse events (TRAE), severe AEs, and withdrawal due to AEs was balanced
between groups.
Overall, there is significant heterogeneity in advanced posterior HR+ breast cancer, while endocrine monotherapy efficacy is limited
.
Therefore, although the results of acelERA research results are not satisfactory, the efficacy is still observed to be prolonged, especially in the ESR1 mutation population, the efficacy trend is more obvious, and the safety is better, which provides a basis
for future research design.
Fig.
5 Secondary efficacy endpoint results of acelERA study
Yimaitong: The new oral SERD has revolutionized the treatment model of breast cancer, but the development of SERD drugs has not been smooth
.
Amcenestrant's Phase 2 AMEERA-3 clinical trial failed to reach the primary endpoint of improving ER+/HER2-mBC advanced second-line or multi-line PFS, and Elacetrian showed significant improvement in PFS in ER+/HER2-mBC second-line and above patients.
Oral SERD has always been a hot spot
.
Although some drug phased studies have reported negative results recently, the SERD drug itself is still widely distributed, and the efficacy in breast cancer is still worth looking forward to
。 Overall, multiple oral SERD are under development, including Roche Giredestrant, AZ Camizestrant, Sanofi Amcenestrant, Radius Elacestrant and Eli Lilly Imlunestrant, and layout HR+/HER2-breast cancer treatment at various stages, such as adjuvant therapy, advanced first-line and advanced second-line + therapy
。 Elacestrant for Radius is currently the first oral SERD
to achieve positive results in CDK4/6 inhibitor treated 2nd line + patients.
In the EMERALD study¹¹ presented at the 2021 SABCS Annual Meeting, intention-to-treat (ITT) and ESR1 mutant populations reached a co-primary endpoint, with PFS benefits primarily driven by ESR1 mutant populations, with median PFS of 3.
8 and 1.
9 months and 1.
9 months and Δ1.
9 months
in the Elacestrant versus control groups, respectively.
At present, Elacetrist has been submitted to the FDA for priority review, but there are no plans to go to the first or auxiliary stage of research and development, and there are no plans
to go public in China.
In August of this year, Sanofi abruptly announced the termination of all clinical development plans for its oral SERD Amcenestrant, a decision based on the AMEERA-5 study (first-line Amcenestrant + pibociclib vs letrozole + pibociclib) Independent Data Monitoring Committee (IDMC) found that the Amcenestrant combined with pibociclib group did not meet the preset boundary for study continuation¹²
。 The results of the AMEERA-3 study¹³ published by ESMO this year showed that the median HR of PFS in the ITT population was 1.
05 and Δ -0.
1 months; In addition, the newly assisted AMEERA-4 study¹⁴ (Amcenestrant vs AI) did not meet the primary study endpoint
.
Based on all of the above, Sanofi halted Amcenestrant's global clinical development program
.
However, this does not affect the confidence of
Giredestrant's development.
Although both Giredestrant and Amcenestrant are oral SERDs, they differ in several key ways: First, in terms of potency, Giredestrant has higher preclinical potency than Amcenestrant; Secondly, in terms of drug interaction (DDI), phase I studies have found that there is a clinically relevant DDI between Amcenestrant and pibociclib, and in the follow-up AMEERA-5 study, the dose of Amcenestrant is reduced from the standard 400mg to 200mg with pibociclib, and its efficacy will inevitably be greatly reduced; Giredestrant, as well as oral SARDs of AZ and Eli Lilly, are DDI-free with pipebociclib; In terms of the third efficacy, the randomized phase 2 study of CoopERA for breast cancer reached its primary endpoint, and compared with AI, Ki-67 decreased more significantly in Giredestrant for 2 weeks, and the inhibitory effect of Ki-67 was maintained until surgery after combination with pibociclib; In the advanced 2-line + acelERA BC study of advanced breast cancer, the HR of Giredestrant vs endocrine monotherapy was 0.
81 and the HR of the ESR1 mutant population was 0.
60, although the study design and baseline characteristics were not the same in different studies, and the cross-interpretation of the study should be interpreted with caution and the performance
of subsequent oral SERD should be expected.
As mentioned earlier, outcomes vary between oral SERDs
.
Overall, we are still looking forward to the new oral SERD, and Elacestrant has obtained FDA priority review designation, and we hope that Giredestrant will bring better news
in the near future.
Moreover, as the only oral SERD in the auxiliary field that is still conducting research, we look forward to more wonderful data disclosure
from Giredestrant.
Overall, the new oral SERD is coming with an unstoppable trend, the dawn has appeared, and it is expected to change the treatment pattern of HR+ breast cancer and bring new hope
to patients.
References:
1.
Kevin K, et al.
ASCO 2022.
LBA1004.
2.
Robertson JF & Harrison M.
Br J Cancer.
2004; 90:S7–10.
3.
Guan J, et al.
Cell.
2019 Aug 8; 178(4):949-963.
4.
Jhaveri K, et al.
ASCO 2021.
Abstract 1017.
5.
Jhaveri K, et al.
SABCS 2020.
Abstract PD7-05.
6.
van Kruchten M, et al.
Cancer discovery.
2015; 5:72–81.
7.
Hurvitz SA, ef al.
SABCS 2021.
Abstract PD-13-06.
8.
Peter A Fasching, et al.
ASCO 2022.
Abstract 589.
9.
Aditya Bardia, et al.
ESMO 2022.
Abstract 144P.
10.
Miguel Martín, et al.
ESMO 2022.
Abstract 211MO.
11.
Aditya Bardia, et al.
SABCS 2021.
Abstract GS2-02.
12.
style="text-align:justify;line-height: 1.
75em;">13.
Tolaney SM, et al.
ESMO 2022.
Abstract 212MO.
14.
Mario Campone, et al.
ASCO 2022.
Abstract 528.
Editor: Max
Review: Max
Typesetting: Youshi
Execution: Traveler
#Professor Zhang Qingyuan of 【Daigoyin】: The final analysis results of the PUFFIN study are released, and the HER2-positive breast cancer treatment is Xinhuazhang!
#Professor Xu Fei of Daigo: Tripa double-target subcutaneous preparations lead a new change in the treatment mode of HER2-positive breast cancer
precision targeted therapy for breast cancer END